
21 Aug My feet are flat, now what?
We previously pointed out that flatfeet can cause malalignment in the joints and abnormal wear to the cartilage in those joints which leads to early onset arthritis. Flatfeet can also cause tendons to work outside of their normal design, which leads to tendonitis and possible rupture. Conservative treatments are highly successful in treating flatfeet. Most patients get excellent relief of their pain caused by the flatfeet with custom orthotics and supportive shoes. Custom orthotics bring a fresh remodel to the floor, giving you better support with every step. The benefit lies in the fact that we build up the floor to the foot, so the foot does not have to collapse to the floor. The orthotic is your own personal custom floor that you get to walk on with every step. With, as with anything, custom orthotics have their limitations as well. When is it time to pursue rebuilding the flat foot?
What are the facts about flatfoot reconstruction?
The foot is the foundation of the body. A moderately active person who takes about 7500 steps per day could potentially take over 200 million steps in a lifetime. The goal behind flatfoot reconstruction is to realign the foot with the leg. In essence, we secure the foundation so the foot can better handle the stresses of everyday life.
I find it really interesting that our society has no fears or issues with correcting crooked teeth, but when it comes to correcting crooked feet, it is almost taboo to speak of. Some studies have reported success rate of flatfoot reconstruction reaching as high as 94%. Other studies have shown that the best time to take on left foot reconstruction is in adolescence. However, studies also show that flatfoot reconstructions in adults are highly successful as well. Reconstructing the flatfoot is not a simple procedure but can lead to lifelong improvement in overall wellbeing.
When should I consider flatfoot reconstruction?
While every case is unique, surgery is most often appropriate in patients with:
- Flat feet diagnosed by X-ray
- Lack of response to conservative methods
- Consistent orthopedic pain
- Loss of ability to carry out regular activities due to flat feet
- Torn or ruptured tendons
Most of the above bullet points applied to pediatric surgery as well. In addition, we also asked questions on whether the child is as active as one would expect relative to his or her peer group. When the child refuses to do fun activities most other kids would not hesitate to do because her feet are tired, this is a cause for concern. Maybe their flatfeet are painful, but they do not know how to express it yet.
What is flatfoot reconstruction?
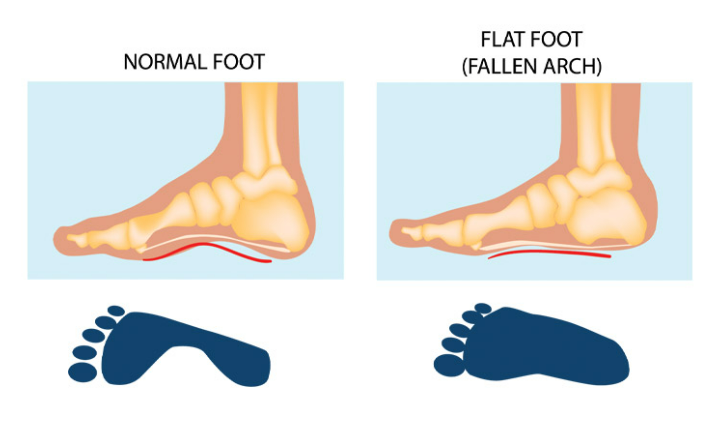
The phrase flatfoot reconstruction can sound a bit overwhelming. When we think about reconstruction, we may envision a house being totally torn apart and put back together and remodeled. Not so much for a flatfoot. We typically use 2 broad categories for flatfeet. A rigid flatfoot versus a flexible flatfoot has different approaches. Most kids are dealing with a flexible flatfoot deformity.
A flexible flatfoot deformity is usually abnormal positioning the bones with weightbearing. There are usually 4 components:
- Short Achilles tendon
- A forefoot that collapses to the outside or laterally
- A midfoot that collapses down
- A heel that turns to the outside or is in valgus.
Depending on what may be present of these four deformities, we address each individual deformity in a stepwise manner. A short Achilles tendon is addressed by an Achilles tendon lengthening. Most often this is accomplished via a minimally invasive incision. A forefoot that collapses to the outside or laterally is addressed with a cut in the heel bone and a wedge added. This procedure is called in Evans calcaneal osteotomy. It also helps reposition the foot in a more neutral position. A midfoot that collapses down can be addressed with another cut in the cuneiform or midfoot which is then filled with a wedge. This brings the forefoot down to the ground and raises the arch. A heel that turns to the outside or is in valgus can be cut in towards the back of the heel and slid to the appropriate position and held in place with screws or pins.
Though the surgery has been around for nearly 50 years, advances in hardware have made the procedure that much more successful. The screws are better designed. The wedges incorporate into the body better than they ever have. We no longer need cadaver bone which has improved the outcomes of the surgeries greatly. By no longer requiring cadaveric bone as a graft, postoperative recovery has improved.
Given the positive outcomes associated with flatfoot reconstruction, there is a time in place where a patient could and should pursue it. As we discussed above, when conservative therapies do not work, or if injury is occurring because of the flatfoot deformity, surgical reconstruction is recommended.
With such a high probability of positive outcomes, a flatfoot reconstruction could greatly improve you or your child’s quality of life, and at Strash Foot & Ankle Care, we are committed to getting you to place your best foot forward, again.